
The patient is a 67 year-old woman with a three week history of erythema, swelling and discomfort of her left lower leg. She had been seen on a number of occasions by her PCP and given cephalexin, but the process persisted. She was evaluated by a dermatologist on April 3, 2025. The left pretibial and calf area were erythematous and indurated. Superficially, there were greyish flaccid bullae. (Figure 1) A bacterial culture was obtained and CBC, CMP and ESR ordered. She was given a prescription for Trimethoprim / Sulfamethoxazole. and a follow-up in two days.
On April 4th the patient became more anxious, contacted her dermatologist and went to the Emergency Room.
There, the E.R. physician performed bedside Point of Care Ultrasound (POCUS) that deonstrated a large non-compressible, non-pulsatile hypoechoic area with irregular borders was above the fascia confirming presence of fluid. Under local Lidocaine with epinephrine anesthesia, the area was aspirated and pus was withdrawn. An incision and drainage was performed yielding copious quantities of creamy pus. The wound was packed with 1” iodoform gauze and i.v. vancomycin was initiated. Wound culture is pending.

Both wound cultures were positive for MRSA, The patient was treated in hospital for two days with i.v. vancomycin and discharged on day three on oral linazolid. Here post I&D course was unventful.
Discussion: When initially seen, the dermatologist was concerned that we were dealing with cellulitis, an evolving ecthyma gangrenosum or pyoderma gangrenosum. Bedside POCUS showed the location of an abscess above the fascia thus pointing towards definitive therapy. Point of Care bedside ultrasound is not a modality most dermatologists are familiar with. In this case, the ER physician was an unappreciated resource.
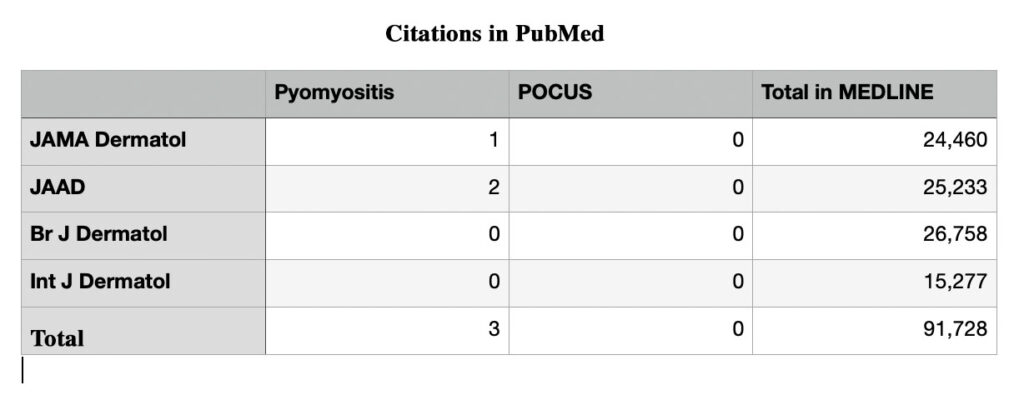
A MEDLINE search retrieved no referenced in the top-tier dermatology journals on ultrasound for skin and soft tissue infections.. PoCUS is not a term dermatologists are familiar with.. The three citations out of 91,728 in MEDLINE is .000032% of the articles a North American dermatologist might see.
Hospital Course:
Reference
1. Koppa BM, Christopher T. Point-of-care ultrasound in skin and soft tissue infections. J Hosp Med 2024 Oct;19(10):938-944. PMID: 39082276
2.Saiag P, Le Breton C, Pavlovic M, Fouchard N, Delzant G, Bigot JM. Magnetic resonance imaging in adults presenting with severe acute infectious cellulitis. Arch Dermatol. 1994 Sep;130(9):1150-8. PMID: 8085870
3. Fox LP, Geyer AS, Grossman ME. Pyomyositis. J Am Acad Dermatol. 2004 Aug;51(2):308-14. doi: 10.1016/j.jaad.2004.01.060. PMID: 15280855
4. Maddox JL Jr, Riordan TP, Odom RB. Pyomyositis in a Neonate. J Am Acad Dermatol. 1984 Feb;10(2 Pt 2):391-4. doi: 10.1016/s0190-9622(84)80014-6. PMID: 6707262
Other useful references:
Squire BT, Fox JC, Anderson C. ABSCESS: applied bedside sonography for convenient evaluation of superficial soft tissue infections. Acad Emerg Med. 2005 Jul;12(7):601-6. PMID: 15995090
Squire BT, Fox JC, Anderson C. ABSCESS: applied bedside sonography for convenient evaluation of superficial soft tissue infections. Acad Emerg Med. 2005 Jul;12(7):601-6. PMID: 15995090
Mulhern CB. Ultrasound, computed tomography and gallium 67 scintigraphy. What they can do and how to use them. Int J Dermatol. 1980 Jun;19(5):279-84. PMID: 7390693